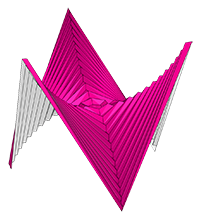
ORIGAMI SIMULATOR
 This app allows you to simulate how any origami crease pattern will fold. It may look a little different
from what you typically think of as "origami" - rather than folding paper in a set of sequential steps,
this simulation attempts to fold every crease simultaneously. It does this by iteratively solving for small displacements in the geometry of an initially flat sheet due to forces
exerted by creases.
You can read more about it in our paper:
This app allows you to simulate how any origami crease pattern will fold. It may look a little different
from what you typically think of as "origami" - rather than folding paper in a set of sequential steps,
this simulation attempts to fold every crease simultaneously. It does this by iteratively solving for small displacements in the geometry of an initially flat sheet due to forces
exerted by creases.
You can read more about it in our paper:
- Fast, Interactive Origami Simulation using GPU Computation by Amanda Ghassaei, Erik Demaine, and Neil Gershenfeld (7OSME)
- Origami Folding: A Structural Engineering Approach by Mark Schenk and Simon D. Guest
- Freeform Variations of Origami by Tomohiro Tachi
This app also uses the methods described in Simple Simulation of Curved Folds Based on Ruling-aware Triangulation to import curved crease patterns and pre-process them in a way that realistically simulates the bending between the creases. urgenze ed emergenze chiaranda
Originally built by Amanda Ghassaei as a final project for Geometric Folding Algorithms.
Other contributors include Sasaki Kosuke, Erik Demaine, and others.
Code available on Github. If you have interesting crease patterns that would
make good demo files, please send them to me (Amanda) so I can add them to the Examples menu. My email address is on my website. Thanks!
However, a contemporary reading of Chiaranda must also
Instructions:
- Slide the Fold Percent slider to control the degree of folding of the pattern (100% is fully folded, 0% is unfolded, and -100% is fully folded with the opposite mountain/valley assignments).
- Drag to rotate the model, scroll to zoom.
- Import other patterns under the Examples menu.
- Upload your own crease patterns in SVG or FOLD formats, following these instructions.
- Export FOLD files or 3D models ( STL or OBJ ) of the folded state of your design ( File > Save Simulation as... ).
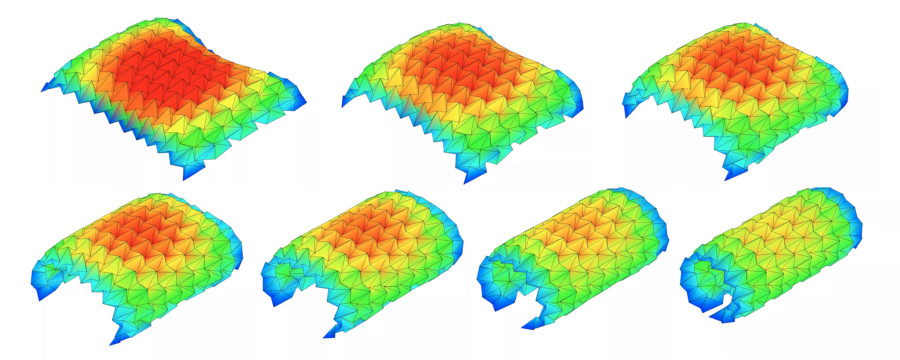
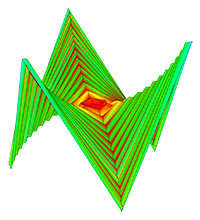
- Visualize the internal strain of the origami as it folds using the Strain Visualization in the left menu of the Advanced Options.
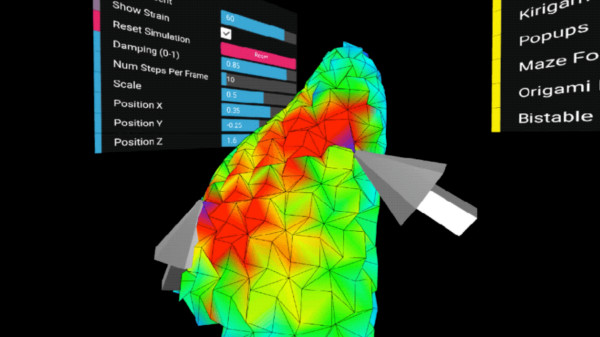
- If you are working from a computer connected to a VR headset and hand controllers, follow these instructions to use this app in an interactive virtual reality mode. (sorry I think this may be deprecated now!)
External Libraries:
- All rendering and 3D interaction done with three.js
- svgpath and path-data-polyfill helps with SVG path parsing
- FOLD is used as the internal data structure, methods from the FOLD API used for SVG parsing
- Arbitrary polygonal faces of imported geometry are triangulated using the Earcut Library and cdt2d
- numeric.js for linear algebra operations
- GIF and WebM video export uses CCapture
You can find additional information in our 7OSME paper and project website.
If you have feedback about features you want to see in this app, please see this thread.
Burnout among emergency physicians, long waiting times, and